A Case of Ocular Melanoma
Nearly 5 years ago a 66 year old healthy woman was having trouble with double vision. For a number of years she felt that her right eye wandered outwards when she was tired or late in the day, and that she was having a harder time controlling it. It was becoming difficult to drive and read. She saw a local eye alignment strabismus surgical specialist who examined her and diagnosed her with a condition known as “alternating exotropia” which was gradually decompensating causing her diplopia. Ocular alignment surgery with extraocular muscle repositioning was recommended to improve the patient’s binocular vision.
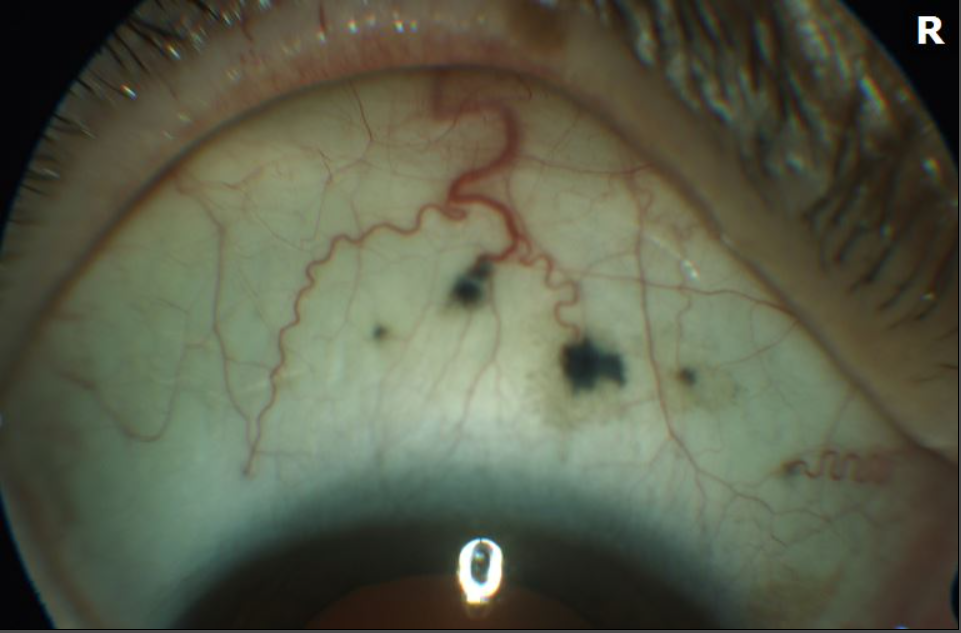
During the careful pre-operative eye exam, there was noted to be a few small dark “spots” on the top surface of the eye, which stood out against the white sclera. These had appeared in the last several months, according to the patient. The eye otherwise appeared to be normal, and her vision was 20/20 in both eyes. Out of caution, the patient was referred to Colorado Retina Associates where she was seen by the Ocular Oncology service, and Ocular Oncologist, Dr. Peter G. Hovland.
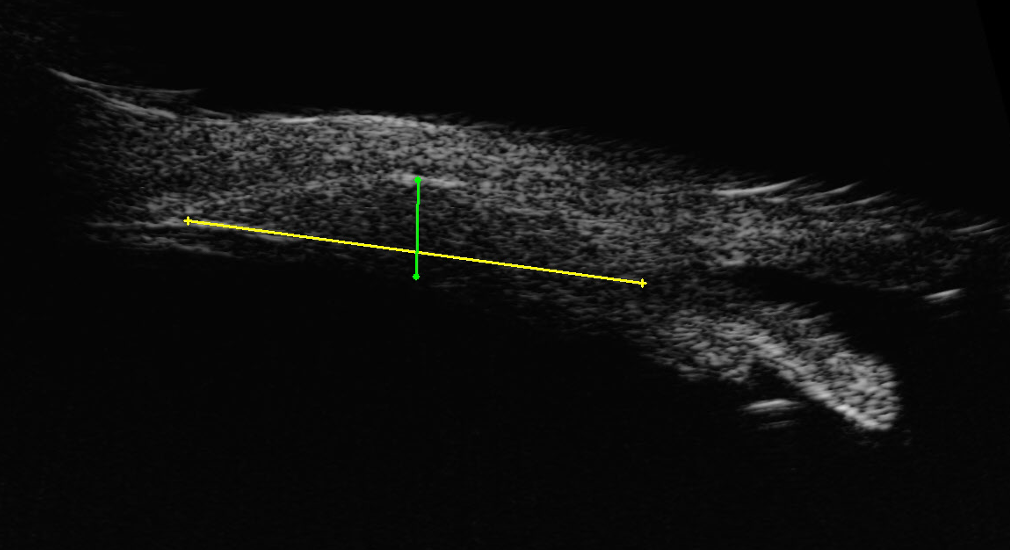
The spotted area of concern was so anterior in the eye that the corresponding internal area could not be easily examined with routine dilation, and a specialized ultrasound was performed to evaluate the internal structure of the wall of the eye. This “anterior b-scan” detected an abnormality. Underneath the pigmented spots of the sclera a tissue mass was found in the ciliary body, which is a ring like anterior structure which is located behind the iris and limbus. She was diagnosed with a melanoma of the ciliary body which was connected to the pigmented spots of the surface.
She was diagnosed with a form of cancer known as ocular melanoma which had started in her eye. This tumor was not only threatening her eye and her vision, but her life as well. Ocular melanoma can spread into the body via the bloodstream known as hematogenous metastasis. Ciliary body melanomas are especially at risk to develop deadly metastases. The patient was entered into the standard protocol to manage patients with ocular melanoma.
An initial “staging” work-up was performed to see if the cancer had already spread in her body even though she had no localizing symptoms. Fortunately, the PET-CT exam found that her body was free of other malignancy. It did however detect a subtle metabolic “activity” in the eye which corresponded to the small tumor suggesting that it was particularly aggressive.
Treatment of ocular melanoma depends on the size and location of the tumor. Large melanomas are treated with enucleation of the eye, yet her tumor was not considered to be large by conventional methods. With the careful ultrasound exam, the tumor size was determined to be 1.2 mm thick with a largest diameter of 9.0 mm and a cross diameter of 5.7 mm. This made it a small melanoma per standard classification. Although such a small tumor could be observed carefully for signs of growth, the concern was that it had already demonstrated an invasive nature, and treatment with radiation was recommended. Consultation with a radiation oncologist was made, and a plan to perform episcleral plaque brachytherapy was created.
The treatment involved two surgeries spaced apart by several days. During the first surgery a careful biopsy of the tumor was performed with a small needle. The sample was sent for molecular prognostic testing. Then a custom designed plaque—a gold-plated implant containing the radioactivity—was attached to the eye in the exact location to deliver a therapeutic dose to the tumor. The eye was carefully covered and she wore a lead eye patch to protect others from the radioactivity. According to exact calculations the treatment timing was determined and she rested at home during the treatment time. The second surgery removed the plaque and restored her eye to normal anatomic structure.
Fortunately, her molecular testing revealed that there was a lower risk that this tumor would metastasize, even though it involved the ciliary body. She gradually recovered for several months, until her eye felt normal again. Over the years of follow-up her tumor gradually shrank, and she continued to have normal results of her body scans. She developed some radiation side effects of the eye which were expected. She had cataract surgery and eventually needed to take glaucoma drops to control her eye pressure. Importantly she even had the strabismus surgery to correct her eye movement and diplopia.
Recently seen on her routine annual follow-up exam, she was nearly five years out from her treatment. Her residual tumor was inactive and her body remained free of metastasis. Her eye alignment was excellent and she had 20/20 vision in both eyes. She was grateful to have put the eye cancer in the past. She felt as healthy as ever and with no double vision has been enjoying playing competitive tennis for the last several years! Her story is a remarkable one which demonstrates the value of teamwork and persistence in our efforts to fight cancer, and the utilization of state of the art ocular surgery to preserve sight and the quality of life which comes with good vision.